Introduction: Hypoglycemia in non-diabetic individuals is rare but represents a significant diagnostic and therapeutic challenge. One of its uncommon causes is Nesidioblastosis, characterized by diffuse or focal hyperplasia of pancreatic β cells, leading to endogenous hyperinsulinemic hypoglycemia. Although more frequent in neonates, cases in adults have been increasingly recognized, especially in the absence of insulinoma. In adults, this condition presents with β cell hypertrophy, enlarged islets, and hyperchromatic nuclei, with postprandial hypoglycemia being its main symptom. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Case Presentation: This article reports the case of a man with intermittent symptomatic hypoglycemia for two years, who required multiple surgical interventions for effective control of the disease. Was done a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to hypoglycemia refractory to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. Discussion and Conclusion: Preoperative diagnosis is challenging due to the nonspecificity of symptoms and the absence of specific functional tests and is usually confirmed by histopathological examination after surgery. Initial treatment involves nutritional modifications and the use of medications. However, moderate to severe and refractory cases require surgical intervention. Partial or subtotal pancreatectomy is effective, although some cases require multiple surgeries. In the reported case, the Frey technique was successfully used, promoting effective glycemic control and minimizing gastrointestinal complications. Despite partial preservation of the pancreas, the patient developed postoperative diabetes, highlighting the importance of balancing effective removal of hyperfunctioning tissue and preservation of pancreatic function. It is concluded that surgical treatment as a last resort and using the technique described by Frey as a way to preserve the gastrointestinal tract and avoid total pancreatectomy with its serious repercussions on the patient's metabolism.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Hypoglycemia in non-diabetic individuals is an uncommon but clinically significant condition that often presents a diagnostic and therapeutic challenge. Among its rare causes, nesidioblastosis stands out as a disorder characterized by diffuse or focal hyperplasia of pancreatic β-cells, leading to endogenous persistent hyperinsulinemic hypoglycemia (PHH). Although more commonly observed in neonates, adult-onset nesidioblastosis has been increasingly recognized, particularly in patients with persistent hypoglycemia and no evidence of insulinoma
[1]
De Leon DD, Arnoux JB, Banerjee I, Bergada I, Bhatti T, Conwell LS, et al. International guidelines for the diagnosis and management of hyperinsulinism. Horm Res Paediatr. 2024; 97(3): 279–98.
. Organic PHH is a disorder of the endocrine pancreas that occurs in newborns and adults. In newborns, PHH is most caused by malfunctioning β-cells, a condition that is known by congenital hyperinsulinism
[2]
Sempoux C, Guiot Y, Jaubert F, Rahier J. Focal and diffuse forms of congenital hyperinsulinism: The keys for differential diagnosis. Endocr Pathol. 2004; 15(3): 241–6.
Heitz PU, Klöppel G, Häcki WH, Polak JM, Pearse AGE. Nesidioblastosis: The pathologic basis of persistent hyperinsulinemic hypoglycemia in infants: Morphologic and quantitative analysis of seven cases based on specific immunostaining and electron microscopy. Diabetes. 1977; 26(7): 632–42.
Goossens A, Gepts W, Saudubray JM, Bonnefont JP, Nihoul-Fekete, Heitz PU, et al. Diffuse and focal nesidioblastosis. A clinicopathological study of 24 patients with persistent neonatal hyperinsulinemic hypoglycemia. Am J Surg Pathol. 1989; 13(9): 766–75.
[5]
DeLellis RA et al. World Health Organization classification of tumours: Pathology and genetics of tumours of endocrine organs. IARC Press. Lyon, 2004.
[4, 5]
. Among adults, PHH can be caused by an insulinoma or, rarely, by Nesidioblastosis
[6]
Fajans SS, Floyd JC Jr. Fasting hypoglycemia in adults. N Engl J Med. 1976; 294(14): 766–72.
Klöppel G, Willemer S, Stamm B, Häcki WH, Heitz PU. Pancreatic lesions and hormonal profile of pancreatic tumors in multiple endocrine neoplasia type I. An immunocytochemical study of nine patients. Cancer. 1986; 57(9): 1824–32.
Reinecke-Lüthge A, Koschoreck F, Klöppel G. The molecular basis of persistent hyperinsulinemic hypoglycemia of infancy and its pathologic substrates. Virchows Arch. 2000; 436(1): 1–5.
Adult patients with Nesidioblastosis, which is characterized by endogenous PHH that is not caused by an insulinoma, have β-cell hypertrophy, islets with enlarged and hyperchromic nuclei, and growing islets that sprout from the periductal epithelium
[9]
Thompson GB, F. John Service, Andrews JC, Lloyd RV, Natt N, van Heerden JA, et al. Noninsulinoma pancreatogenous hypoglycemia syndrome: An update in 10 surgically treated patients. Surgery. 2000; 128(6): 937–45.
Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, et al. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005; 29(4): 524–33.
García-Santos EP, Manzanares-Campillo M del C, Padilla-Valverde D, Villarejo-Campos P, Gil-Rendo A, Muñoz-Atienza V, et al. Nesidioblastosis. A case of hyperplasia of the islets of Langerhans in the adult. Pancreatology. 2013; 13(5): 544–8.
. The predominant clinical feature of this disease is postprandial hypoglycemia and biochemical findings similar to those of insulinoma
[12]
F. John Service, Natt N, Thompson GB, Grant CS, van Heerden JA, Andrews JC, et al. Noninsulinoma pancreatogenous hypoglycemia: A novel syndrome of hyperinsulinemic hypoglycemia in adults independent of mutations in Kir6.2 and SUR1 genes1. J Clin Endocrinol Metab. 1999; 84(5): 1582–9.
Because of this, a case of Nesidioblastosis is reported in an adult male with a two-year history of intermittent episodes of symptomatic hypoglycemia, requiring several surgical interventions for an effective treatment. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to refractory hypoglycemia to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. We will describe the case and the surgical technique employed.
2. Case Presentation
A 47-year-old male patient, with a mean body mass index (BMI) of 41.4 kg/m², started his clinical context in 2012, reporting episodes of loss of consciousness about six to eight times a day, diagnosed by blood glucose test. The symptoms worsened, leading him to seek medical help. The symptoms were investigated and the hypothesis of Nesidioblastosis was raised.
In 2014, he was referred to Hospital Sírio Libanês, where he underwent tests that found Nesidioblastosis affecting the tail and head of the pancreas. Therefore, he started to receive clinical-pharmacological treatment with Diazoxide and Octreotide. However, the patient's symptoms worsened, leading him, in 2015, to a body-caudal pancreatectomy and Roux-en-Y gastric bypass. After the procedure, he reported that he remained asymptomatic for three months, when hypoglycemic symptoms reappeared.
In 2016, the patient presented with semi-intestinal occlusion, requiring two surgical interventions - in one of them, the Roux-en-Y gastric bypass was undone due to intestinal invagination. In 2017, he evolved with severe hypoglycemia, returning to seek specialized medical care. He denied associated comorbidities.
In view of the situation, a selective calcium stimulation test was performed [Figure 1] which showed excess insulin production in the region irrigated by the superior mesenteric artery (SMA) and gastroduodenal artery (GDA).
Figure 1. Selective calcium stimulation test, basal insulin test and 30 and 60 seconds after calcium infusion were performed. In the SMA (A) the values were, respectively, 9.95, 11.78 and 50.02. In the GDA (B) they were, respectively, 2.47, 11.74 and 2.41.
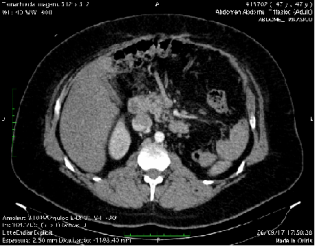
In addition, a computed tomography of the abdomen was performed [Figure 2], which did not show neoplastic processes, with only changes in the abdominal anatomy due to previous surgeries being observed - in addition to the surgeries already mentioned in 2015 and 2016, there was also a partial left nephrectomy for removal of a sarcoma in 1999.
Figure 2. Abdominal CT showing head and uncinate process with pancreas with preserved density, with usual contrast enhancement. Pancreatic body and tail not visible. Post-nephrectomy status.
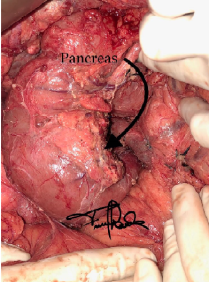
After that, an open surgical reintervention was chosen to reduce the volume of pancreatic tissue still existing through a subtotal pancreatectomy with duodenal preservation. For this, with the patient in the supine position and under general anesthesia, a Chevron laparotomy was performed, with resection of the anterior scar. The next step was the resection of the head and the uncinate process of the pancreas like the Frey technique [figure 3].
Figure 3. Image after surgical procedure using the Frey Technique.
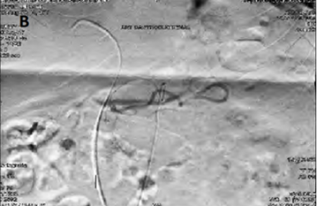
During the procedure, the patient's blood glucose was measured every thirty minutes and after resection of the uncinate process, as well as a sub-total portion of the head of the pancreas, blood glucose increased to levels above 200 mg/dL. Then, biological glue was placed on the resected area and a cholecystectomy and a cholangiography [figure 4] were performed to verify the integrity of the retro-pancreatic bile duct. In addition, an appendectomy was performed and, due to the complexity of the case. The 24 Fr Blake drain was placed close to the resection.
Figure 4. Cholangiography showing the integrity of the intrapancreatic portion of the common bile duct.
In the pathological examination of the seven sections of the pancreas (uncinate process and head) removed during surgery, hyperplasia of pancreatic islets and nuclear hypertrophy of beta cells were observed. In immunohistochemistry, the results were positive for the following antibodies: cytokeratins AE1/AE3, chromogranin A, synaptophysin, CD56 and insulin, being negative for: glucagon and Ki-67. These findings, together with the clinical data, support the diagnosis of Nesidioblastosis.
After the surgical procedure, the patient presented eradication of hypoglycemic episodes, with a controlled diet and using insulin, Dapaglifozin and Pancreatin. During follow-up after the surgical procedure, lasting 8 years, the patient did not present complications associated with the underlying pathology treated, and the monitoring of Insulin basal levels showed between 3,45 mU/ml and 4,25 mU/ml, maintaining high blood glucose levels, controlled with the use of medications described above.
3. Discussion and Conclusions
According to published statistics, 0.5 to 5.0% of nesidioblastosis cases occur in adults
[13]
Witteles RM. Adult-onset nesidioblastosis causing hypoglycemia: An important clinical entity and continuing treatment dilemma. Arch Surg. 2001; 136(6): 656.
, and it is therefore a rare disease among adults that causes hyperinsulinemic hypoglycemia. The first description of a case related to nesidioblastosis occurred in 1938 and was in children
[14]
Sandler R, Horwitz DL, Rubenstein AH, Kuzuya H. Hypoglycemia and endogenous hyperinsulinism complicating diabetes mellitus. Am J Med. 1975; 59(5): 730–6.
. Only in 1975 was the first case described in adults
[15]
Stefanini P, Carboni M, Patrassi N, Basoli A. Beta-islet cell tumors of the pancreas: results of a study on 1,067 cases. Surgery. 1974 Apr; 75(4): 597-609. PMID: 4366135.
[15]
. In this age group, nesidioblastosis is characterized by a functional disorder of beta cells that can occur as a feature of noninsulinoma pancreatogenous hypoglycemia syndrome or after Roux-en-Y gastric bypass surgery, both of which cause endogenous hypoglycemia. However, the most common cause of this condition in adults is local or multiple insulinoma
[16]
Klöppel G, Anlauf M, Raffel A, Perren A, Knoefel WT. Adult diffuse nesidioblastosis: genetically or environmentally induced? Hum Pathol. 2008; 39(1): 3–8.
The predominant clinical feature is postprandial hypoglycemia. In a series of 18 Mayo Clinic patients, aged 16 to 78 years, BMI of 25.7 kg/m², with a male predominance (70%), symptoms occurred postprandially, two to four hours after meals, and rarely fasting
[9]
Thompson GB, F. John Service, Andrews JC, Lloyd RV, Natt N, van Heerden JA, et al. Noninsulinoma pancreatogenous hypoglycemia syndrome: An update in 10 surgically treated patients. Surgery. 2000; 128(6): 937–45.
Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, et al. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005; 29(4): 524–33.
. In contrast, most patients with insulinoma have fasting hypoglycemia. In the case reported, the patient did not present specific moments of hypoglycemic symptoms, which occurred randomly.
The preoperative diagnosis of adult nesidioblastosis is challenging, as there are no determining clinical symptoms or history and there are no highly specific functional tests
[18]
Clancy TE, Moore FD Jr, Zinner MJ. Post-gastric bypass hyperinsulinism with nesidioblastosis: subtotal or total pancreatectomy may be needed to prevent recurrent hypoglycemia. J Gastrointest Surg. 2006; 10(8): 1116–9.
. The patient reported in the case presented unspecific complaints and functional tests were not performed previously, as the patient already had a previous diagnosis of nesidioblastosis. A selective arterial calcium stimulation test can indicate hyperactive β-cell activity and provide guidance for disease localization and direct resection of appropriate pancreatic regions
[19]
Frey CF, Suzuki M, Isaji S, Zhu Y. Pancreatic resection for chronic pancreatitis. Surg Clin North Am. 1989; 69(3): 499–528.
. Such examination determined an increase in insulin production in the regions irrigated by SMA and GDA, which correspond to irrigation of the head and uncinate process.
The diagnostic criteria for adult nesidioblastosis proposed by Klöppel et al
[17]
Raffel A, Krausch M M, Anlauf M, Wieben D, Braunstein S, Klöppel G, et al. Diffuse nesidioblastosis as a cause of hyperinsulinemic hypoglycemia in adults: A diagnostic and therapeutic challenge. Surgery. 2007; 141(2): 179–84.
involve exclusion of an insulinoma and several histological features. Thus, the definitive diagnosis of adult nesidioblastosis is better defined postoperatively after performing a histological examination. All the criteria proposed by Kloppel et al
[17]
Raffel A, Krausch M M, Anlauf M, Wieben D, Braunstein S, Klöppel G, et al. Diffuse nesidioblastosis as a cause of hyperinsulinemic hypoglycemia in adults: A diagnostic and therapeutic challenge. Surgery. 2007; 141(2): 179–84.
were evidenced in the pathological study of the removed piece. In addition, immunohistochemistry also contributed to the diagnosis of nesidioblastosis, since diffuse neuroendocrine tissue was observed.
For the treatment of Nesidioblastosis in patients with mild to moderate symptoms, nutritional modification is a reasonable initial intervention. Nutritional modification particularly reducing high absorption free carbohydrate. If mild to moderate symptoms persist, we prescribe Acarbose, an alpha-glucosidase inhibitor. Other medications such as: Octreotides, Verapamil, Diazoxide and Acarbose improved symptoms of hypoglycemia in patients after Roux-en-Y bypass.
However, the definitive treatment for severe and moderate cases of refractory hypoglycemia to other therapies is the surgical procedure, avoiding relapses in clinical treatment and subsequent complications due to delayed surgical management
[20]
Thapa S, Kaur K, Yadav GK, Kumari D, Phulware RH. Non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS)/Nesidioblastosis as the underlying cause of recurrent hypoglycemia in a diabetic adult. Autops Case Rep. 2023; 13: e2023451.
. As the patient in this report was not successful with the clinical treatment initially proposed, surgical intervention was chosen. Although there is no standard surgical technique, partial or subtotal pancreatectomy was able to resolve most cases
[9]
Thompson GB, F. John Service, Andrews JC, Lloyd RV, Natt N, van Heerden JA, et al. Noninsulinoma pancreatogenous hypoglycemia syndrome: An update in 10 surgically treated patients. Surgery. 2000; 128(6): 937–45.
Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, et al. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005; 29(4): 524–33.
However, some required multiple surgical interventions due to symptoms of recurrent hypoglycemia after surgery
[21]
Dieterle MP, Husari A, Prozmann SN, Wiethoff H, Stenzinger A, Röhrich M, et al. An uncommon cause of recurrent presyncope, dizziness, and tachycardia: A case report of diffuse, adult-onset nesidioblastosis/non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS). Biomedicines. 2023; 11(6).
Cao J, Kim C, Huynh T, Frugoli A, Henson H, Valdez V, et al. BYPASS-OMA: Hypoglycemic hyperinsulinemic nesidioblastosis after gastric bypass surgery-A case report and review of the literature. Case Rep Endocrinol. 2022; 2022: 5472304.
Due to these multiple interventions, the extent of pancreatic resection requires caution to preserve sufficient β-cell volume to prevent diabetes. In the reported case, the patient behaved similarly, since he needed two approaches, the latter being a subtotal pancreatectomy with duodenal preservation, based on the Frey technique, proposed by Frey et al
[19]
Frey CF, Suzuki M, Isaji S, Zhu Y. Pancreatic resection for chronic pancreatitis. Surg Clin North Am. 1989; 69(3): 499–528.
for the treatment of chronic pancreatitis. Such intervention, proved to be effective and reduced the patient's symptoms and helped in glycemic control since the patient had a small part of the pancreas still preserved. This approach avoids postoperative complications and reduce the risk of morbidity and mortality from more invasive procedures that can be used to manage Nesidioblastosis
[21]
Dieterle MP, Husari A, Prozmann SN, Wiethoff H, Stenzinger A, Röhrich M, et al. An uncommon cause of recurrent presyncope, dizziness, and tachycardia: A case report of diffuse, adult-onset nesidioblastosis/non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS). Biomedicines. 2023; 11(6).
Cao J, Kim C, Huynh T, Frugoli A, Henson H, Valdez V, et al. BYPASS-OMA: Hypoglycemic hyperinsulinemic nesidioblastosis after gastric bypass surgery-A case report and review of the literature. Case Rep Endocrinol. 2022; 2022: 5472304.
Thus, it is evident that the surgical technique used (Frey's technique) was efficient for the patient's glycemic control and without sequelae to the gastrointestinal tract, however, despite the preservation of pancreatic tissue, the reported case developed diabetes after pancreatic tissue resections.
Abbreviations
PHH
Persistent Hyperinsulinemic Hypoglycemia
BMI
Body Mass Index
SMA
Superior Mesenteric Artery
GDA
Gastroduodenal Artery
Ethics Approval
The study followed the ethical and legal standards recommended by Resolution 466/12 of the National Health Council and was approved by the Research Ethics Committee of the Onofre Lopes University Hospital. Written informed consent was obtained from the patient for publication of the details of his medical case and any accompanying images.
Author Contributions
Fernando Freire Lisboa: Investigation, Methodology, Writing – original draft
Fernando Freire Lisboa Junior: Project administration, Resources
Luis Fernando Nunes Ferreira: Methodology,Resources,Writing – review & editing
Gabriel Diniz Câmara Dantas: Methodology, Resources, Writing – original draft
Gabriel Carvalho de Oliveira Cruz: Investigation, Writing – original draft
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
De Leon DD, Arnoux JB, Banerjee I, Bergada I, Bhatti T, Conwell LS, et al. International guidelines for the diagnosis and management of hyperinsulinism. Horm Res Paediatr. 2024; 97(3): 279–98.
Sempoux C, Guiot Y, Jaubert F, Rahier J. Focal and diffuse forms of congenital hyperinsulinism: The keys for differential diagnosis. Endocr Pathol. 2004; 15(3): 241–6.
Heitz PU, Klöppel G, Häcki WH, Polak JM, Pearse AGE. Nesidioblastosis: The pathologic basis of persistent hyperinsulinemic hypoglycemia in infants: Morphologic and quantitative analysis of seven cases based on specific immunostaining and electron microscopy. Diabetes. 1977; 26(7): 632–42.
Goossens A, Gepts W, Saudubray JM, Bonnefont JP, Nihoul-Fekete, Heitz PU, et al. Diffuse and focal nesidioblastosis. A clinicopathological study of 24 patients with persistent neonatal hyperinsulinemic hypoglycemia. Am J Surg Pathol. 1989; 13(9): 766–75.
[5]
DeLellis RA et al. World Health Organization classification of tumours: Pathology and genetics of tumours of endocrine organs. IARC Press. Lyon, 2004.
[6]
Fajans SS, Floyd JC Jr. Fasting hypoglycemia in adults. N Engl J Med. 1976; 294(14): 766–72.
Klöppel G, Willemer S, Stamm B, Häcki WH, Heitz PU. Pancreatic lesions and hormonal profile of pancreatic tumors in multiple endocrine neoplasia type I. An immunocytochemical study of nine patients. Cancer. 1986; 57(9): 1824–32.
Reinecke-Lüthge A, Koschoreck F, Klöppel G. The molecular basis of persistent hyperinsulinemic hypoglycemia of infancy and its pathologic substrates. Virchows Arch. 2000; 436(1): 1–5.
Thompson GB, F. John Service, Andrews JC, Lloyd RV, Natt N, van Heerden JA, et al. Noninsulinoma pancreatogenous hypoglycemia syndrome: An update in 10 surgically treated patients. Surgery. 2000; 128(6): 937–45.
Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, et al. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005; 29(4): 524–33.
García-Santos EP, Manzanares-Campillo M del C, Padilla-Valverde D, Villarejo-Campos P, Gil-Rendo A, Muñoz-Atienza V, et al. Nesidioblastosis. A case of hyperplasia of the islets of Langerhans in the adult. Pancreatology. 2013; 13(5): 544–8.
F. John Service, Natt N, Thompson GB, Grant CS, van Heerden JA, Andrews JC, et al. Noninsulinoma pancreatogenous hypoglycemia: A novel syndrome of hyperinsulinemic hypoglycemia in adults independent of mutations in Kir6.2 and SUR1 genes1. J Clin Endocrinol Metab. 1999; 84(5): 1582–9.
Stefanini P, Carboni M, Patrassi N, Basoli A. Beta-islet cell tumors of the pancreas: results of a study on 1,067 cases. Surgery. 1974 Apr; 75(4): 597-609. PMID: 4366135.
[16]
Klöppel G, Anlauf M, Raffel A, Perren A, Knoefel WT. Adult diffuse nesidioblastosis: genetically or environmentally induced? Hum Pathol. 2008; 39(1): 3–8.
Raffel A, Krausch M M, Anlauf M, Wieben D, Braunstein S, Klöppel G, et al. Diffuse nesidioblastosis as a cause of hyperinsulinemic hypoglycemia in adults: A diagnostic and therapeutic challenge. Surgery. 2007; 141(2): 179–84.
Clancy TE, Moore FD Jr, Zinner MJ. Post-gastric bypass hyperinsulinism with nesidioblastosis: subtotal or total pancreatectomy may be needed to prevent recurrent hypoglycemia. J Gastrointest Surg. 2006; 10(8): 1116–9.
Thapa S, Kaur K, Yadav GK, Kumari D, Phulware RH. Non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS)/Nesidioblastosis as the underlying cause of recurrent hypoglycemia in a diabetic adult. Autops Case Rep. 2023; 13: e2023451.
Dieterle MP, Husari A, Prozmann SN, Wiethoff H, Stenzinger A, Röhrich M, et al. An uncommon cause of recurrent presyncope, dizziness, and tachycardia: A case report of diffuse, adult-onset nesidioblastosis/non-insulinoma pancreatogenous hypoglycemia syndrome (NIPHS). Biomedicines. 2023; 11(6).
Cao J, Kim C, Huynh T, Frugoli A, Henson H, Valdez V, et al. BYPASS-OMA: Hypoglycemic hyperinsulinemic nesidioblastosis after gastric bypass surgery-A case report and review of the literature. Case Rep Endocrinol. 2022; 2022: 5472304.
Lisboa, F. F., Junior, F. F. L., Ferreira, L. F. N., Dantas, G. D. C., Cruz, G. C. D. O. (2025). Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. Journal of Surgery, 13(3), 45-50. https://doi.org/10.11648/j.js.20251303.11
Lisboa, F. F.; Junior, F. F. L.; Ferreira, L. F. N.; Dantas, G. D. C.; Cruz, G. C. D. O. Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. J. Surg.2025, 13(3), 45-50. doi: 10.11648/j.js.20251303.11
Lisboa FF, Junior FFL, Ferreira LFN, Dantas GDC, Cruz GCDO. Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. J Surg. 2025;13(3):45-50. doi: 10.11648/j.js.20251303.11
@article{10.11648/j.js.20251303.11,
author = {Fernando Freire Lisboa and Fernando Freire Lisboa Junior and Luis Fernando Nunes Ferreira and Gabriel Diniz Câmara Dantas and Gabriel Carvalho de Oliveira Cruz},
title = {Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report},
journal = {Journal of Surgery},
volume = {13},
number = {3},
pages = {45-50},
doi = {10.11648/j.js.20251303.11},
url = {https://doi.org/10.11648/j.js.20251303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251303.11},
abstract = {Introduction: Hypoglycemia in non-diabetic individuals is rare but represents a significant diagnostic and therapeutic challenge. One of its uncommon causes is Nesidioblastosis, characterized by diffuse or focal hyperplasia of pancreatic β cells, leading to endogenous hyperinsulinemic hypoglycemia. Although more frequent in neonates, cases in adults have been increasingly recognized, especially in the absence of insulinoma. In adults, this condition presents with β cell hypertrophy, enlarged islets, and hyperchromatic nuclei, with postprandial hypoglycemia being its main symptom. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Case Presentation: This article reports the case of a man with intermittent symptomatic hypoglycemia for two years, who required multiple surgical interventions for effective control of the disease. Was done a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to hypoglycemia refractory to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. Discussion and Conclusion: Preoperative diagnosis is challenging due to the nonspecificity of symptoms and the absence of specific functional tests and is usually confirmed by histopathological examination after surgery. Initial treatment involves nutritional modifications and the use of medications. However, moderate to severe and refractory cases require surgical intervention. Partial or subtotal pancreatectomy is effective, although some cases require multiple surgeries. In the reported case, the Frey technique was successfully used, promoting effective glycemic control and minimizing gastrointestinal complications. Despite partial preservation of the pancreas, the patient developed postoperative diabetes, highlighting the importance of balancing effective removal of hyperfunctioning tissue and preservation of pancreatic function. It is concluded that surgical treatment as a last resort and using the technique described by Frey as a way to preserve the gastrointestinal tract and avoid total pancreatectomy with its serious repercussions on the patient's metabolism.
},
year = {2025}
}
TY - JOUR
T1 - Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report
AU - Fernando Freire Lisboa
AU - Fernando Freire Lisboa Junior
AU - Luis Fernando Nunes Ferreira
AU - Gabriel Diniz Câmara Dantas
AU - Gabriel Carvalho de Oliveira Cruz
Y1 - 2025/05/29
PY - 2025
N1 - https://doi.org/10.11648/j.js.20251303.11
DO - 10.11648/j.js.20251303.11
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 45
EP - 50
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20251303.11
AB - Introduction: Hypoglycemia in non-diabetic individuals is rare but represents a significant diagnostic and therapeutic challenge. One of its uncommon causes is Nesidioblastosis, characterized by diffuse or focal hyperplasia of pancreatic β cells, leading to endogenous hyperinsulinemic hypoglycemia. Although more frequent in neonates, cases in adults have been increasingly recognized, especially in the absence of insulinoma. In adults, this condition presents with β cell hypertrophy, enlarged islets, and hyperchromatic nuclei, with postprandial hypoglycemia being its main symptom. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Case Presentation: This article reports the case of a man with intermittent symptomatic hypoglycemia for two years, who required multiple surgical interventions for effective control of the disease. Was done a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to hypoglycemia refractory to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. Discussion and Conclusion: Preoperative diagnosis is challenging due to the nonspecificity of symptoms and the absence of specific functional tests and is usually confirmed by histopathological examination after surgery. Initial treatment involves nutritional modifications and the use of medications. However, moderate to severe and refractory cases require surgical intervention. Partial or subtotal pancreatectomy is effective, although some cases require multiple surgeries. In the reported case, the Frey technique was successfully used, promoting effective glycemic control and minimizing gastrointestinal complications. Despite partial preservation of the pancreas, the patient developed postoperative diabetes, highlighting the importance of balancing effective removal of hyperfunctioning tissue and preservation of pancreatic function. It is concluded that surgical treatment as a last resort and using the technique described by Frey as a way to preserve the gastrointestinal tract and avoid total pancreatectomy with its serious repercussions on the patient's metabolism.
VL - 13
IS - 3
ER -
Lisboa, F. F., Junior, F. F. L., Ferreira, L. F. N., Dantas, G. D. C., Cruz, G. C. D. O. (2025). Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. Journal of Surgery, 13(3), 45-50. https://doi.org/10.11648/j.js.20251303.11
Lisboa, F. F.; Junior, F. F. L.; Ferreira, L. F. N.; Dantas, G. D. C.; Cruz, G. C. D. O. Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. J. Surg.2025, 13(3), 45-50. doi: 10.11648/j.js.20251303.11
Lisboa FF, Junior FFL, Ferreira LFN, Dantas GDC, Cruz GCDO. Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report. J Surg. 2025;13(3):45-50. doi: 10.11648/j.js.20251303.11
@article{10.11648/j.js.20251303.11,
author = {Fernando Freire Lisboa and Fernando Freire Lisboa Junior and Luis Fernando Nunes Ferreira and Gabriel Diniz Câmara Dantas and Gabriel Carvalho de Oliveira Cruz},
title = {Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report},
journal = {Journal of Surgery},
volume = {13},
number = {3},
pages = {45-50},
doi = {10.11648/j.js.20251303.11},
url = {https://doi.org/10.11648/j.js.20251303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251303.11},
abstract = {Introduction: Hypoglycemia in non-diabetic individuals is rare but represents a significant diagnostic and therapeutic challenge. One of its uncommon causes is Nesidioblastosis, characterized by diffuse or focal hyperplasia of pancreatic β cells, leading to endogenous hyperinsulinemic hypoglycemia. Although more frequent in neonates, cases in adults have been increasingly recognized, especially in the absence of insulinoma. In adults, this condition presents with β cell hypertrophy, enlarged islets, and hyperchromatic nuclei, with postprandial hypoglycemia being its main symptom. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Case Presentation: This article reports the case of a man with intermittent symptomatic hypoglycemia for two years, who required multiple surgical interventions for effective control of the disease. Was done a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to hypoglycemia refractory to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. Discussion and Conclusion: Preoperative diagnosis is challenging due to the nonspecificity of symptoms and the absence of specific functional tests and is usually confirmed by histopathological examination after surgery. Initial treatment involves nutritional modifications and the use of medications. However, moderate to severe and refractory cases require surgical intervention. Partial or subtotal pancreatectomy is effective, although some cases require multiple surgeries. In the reported case, the Frey technique was successfully used, promoting effective glycemic control and minimizing gastrointestinal complications. Despite partial preservation of the pancreas, the patient developed postoperative diabetes, highlighting the importance of balancing effective removal of hyperfunctioning tissue and preservation of pancreatic function. It is concluded that surgical treatment as a last resort and using the technique described by Frey as a way to preserve the gastrointestinal tract and avoid total pancreatectomy with its serious repercussions on the patient's metabolism.
},
year = {2025}
}
TY - JOUR
T1 - Modified Frey Technique for Treatment of Persistent Hyperinsulinemic Hipoglicemia Due to Nesidioblastosis: A Case Report
AU - Fernando Freire Lisboa
AU - Fernando Freire Lisboa Junior
AU - Luis Fernando Nunes Ferreira
AU - Gabriel Diniz Câmara Dantas
AU - Gabriel Carvalho de Oliveira Cruz
Y1 - 2025/05/29
PY - 2025
N1 - https://doi.org/10.11648/j.js.20251303.11
DO - 10.11648/j.js.20251303.11
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 45
EP - 50
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20251303.11
AB - Introduction: Hypoglycemia in non-diabetic individuals is rare but represents a significant diagnostic and therapeutic challenge. One of its uncommon causes is Nesidioblastosis, characterized by diffuse or focal hyperplasia of pancreatic β cells, leading to endogenous hyperinsulinemic hypoglycemia. Although more frequent in neonates, cases in adults have been increasingly recognized, especially in the absence of insulinoma. In adults, this condition presents with β cell hypertrophy, enlarged islets, and hyperchromatic nuclei, with postprandial hypoglycemia being its main symptom. This article aims to demonstrate a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Case Presentation: This article reports the case of a man with intermittent symptomatic hypoglycemia for two years, who required multiple surgical interventions for effective control of the disease. Was done a technical modification for preserving the duodenum and bile duct in the treatment of a patient with Nesidioblastosis who underwent several surgical treatments without results. Given the current clinical picture, in which a pancreaticoduodenectomy with total resection of the remaining pancreas would be indicated due to hypoglycemia refractory to several types of clinical and surgical treatments, we decided to perform the Frey technique for this case, thus preserving a small segment of the pancreas together with the duodenal arch and thus preserving the main bile duct. Discussion and Conclusion: Preoperative diagnosis is challenging due to the nonspecificity of symptoms and the absence of specific functional tests and is usually confirmed by histopathological examination after surgery. Initial treatment involves nutritional modifications and the use of medications. However, moderate to severe and refractory cases require surgical intervention. Partial or subtotal pancreatectomy is effective, although some cases require multiple surgeries. In the reported case, the Frey technique was successfully used, promoting effective glycemic control and minimizing gastrointestinal complications. Despite partial preservation of the pancreas, the patient developed postoperative diabetes, highlighting the importance of balancing effective removal of hyperfunctioning tissue and preservation of pancreatic function. It is concluded that surgical treatment as a last resort and using the technique described by Frey as a way to preserve the gastrointestinal tract and avoid total pancreatectomy with its serious repercussions on the patient's metabolism.
VL - 13
IS - 3
ER -